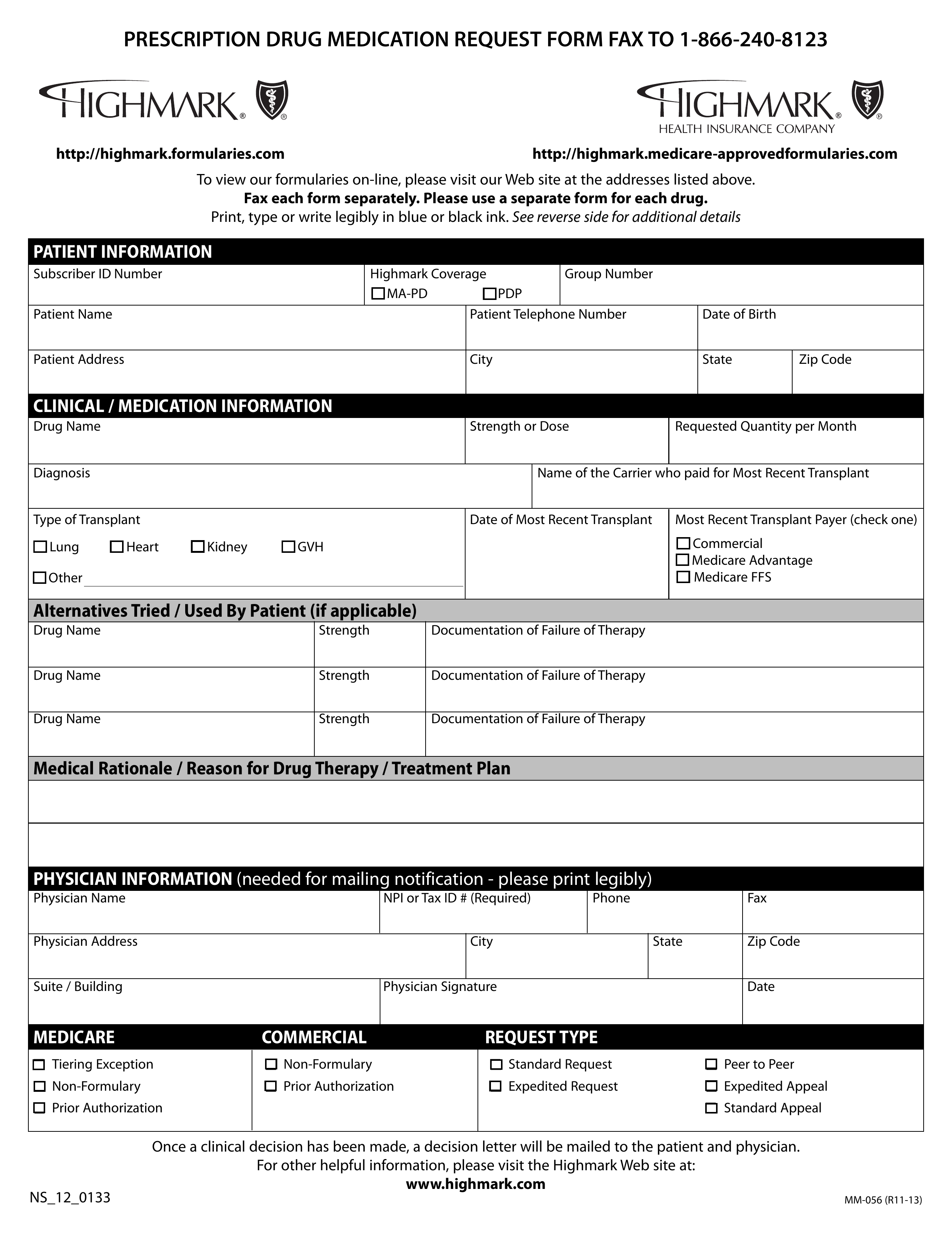
Weve provided the following resources to help you understand Anthems prior authorization process and obtain authorization for your patients when its required. Medical Management Policy 120 Fifth Avenue MC P4207 Pittsburgh PA 15222.
 Fillable Online Illinois Medicare One Pre Authorization Form Fax Email Print Pdffiller
Fillable Online Illinois Medicare One Pre Authorization Form Fax Email Print Pdffiller
Prior Authorization Form Xolair Buy-and-bill requests for this drug should be submitted through NaviNet.

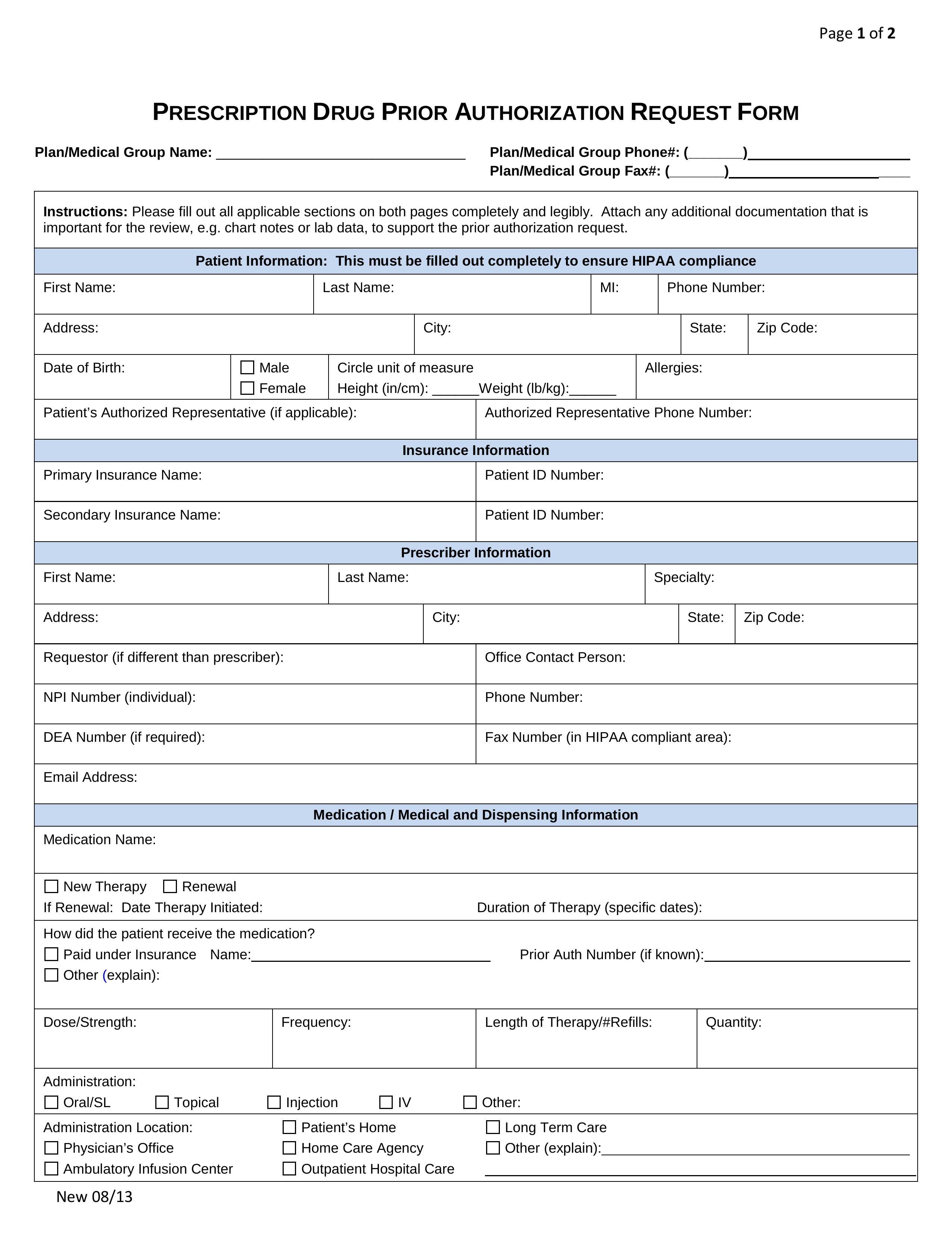
Highmark prior authorization form. Chronic Inflammatory Diseases Medication Request Form. If you do not obtain prior approval there may be a reduction or denial of your benefit. This is called prior approval precertification or preauthorization.
The Appeals Administrator from the. Urgentemergency admissions do not require prior authorization. Effective November 1 2020 Highmark is expanding our prior authorization requirements for outpatient services to include those services provided by out-of-area providers participating with their local Blue Plan.
ONLY COMPLETED REQUESTS WILL BE REVIEWED. 1 866 240-8123 Mail. Some authorization requirements vary by member contract.
In-Network Referral Form Fillable form for fax use. Use this form to request authorization by fax or mail when a n issuer requires prior authorization of a health care service. Highmark Prior Rx Authorization Form Fax.
Form Title Networks Expedited Pre-service Clinical Appeal Form. The Anthem Blue Cross Blue Shield prior authorization form is what physicians will use when requesting payment for a patients prescription cost. Employees submitting an appeal without a signed Authorization Form andor completed Health Plan Appeal Form and Checklist will be requested in writing to submit the forms.
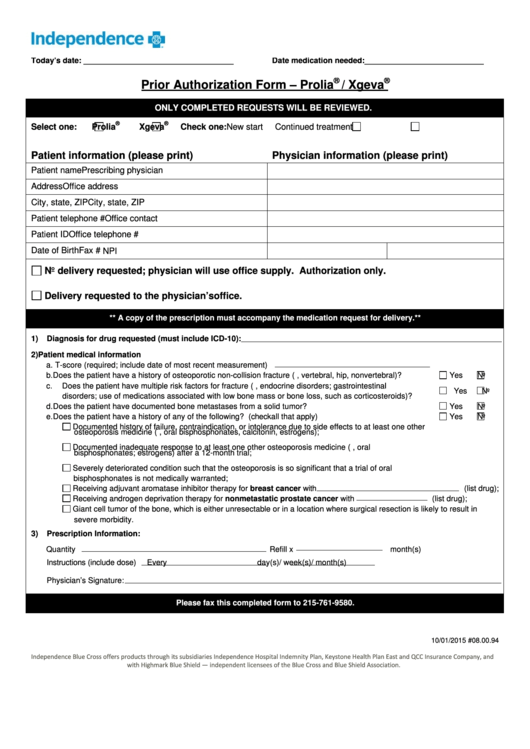
M New start M Continued treatment Patient information please print Physician information please print Patient name Prescribing physician Address Office address. 4152018 080100 Independence Blue Cross offers products directly through its subsidiaries Keystone Health Plan East and QCC Insurance Company and with Highmark Blue Shield independent licensees of the Blue Cross and Blue Shield Association. Obtaining a prior authorization helps us pay claims faster with no denied charges or unexpected costs to our members.
Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form. 28 rijen A standardized or uniform prior authorization PA form may be. Blood Disorders Medication Request Form.
Pharmacy Prior Authorization Forms. Statewide Benefits Office will not begin to review the appeal until the Authorization Form and the Appeal Form and Checklist are received. Prior Authorization Health insurance can be complicatedespecially when it comes to prior authorization also referred to as pre-approval pre-authorization and pre-certification.
Extended Release Opioid Prior Authorization Form. The authorization is typically obtained by the ordering provider. We review them to ensure they are medically necessary.
Provider Forms Guides Easily find and download forms guides and other related documentation that you need to do business with Anthem all in one convenient location. CGRP Inhibitors Medication Request Form. Home Health Care Preauthorization Form.
Some services require prior authorization preauthorization before they are performed. 855 476-4158 If needed you may call to speak to a Pharmacy Services Representative. PRIOR AUTHORIZATION FORM Please complete and fax all requested information below including any progress notes laboratory test results or chart documentation as applicable to Highmark Health Options Pharmacy Services.
We are currently in the process of enhancing this forms library. Please fax this completed form to 215-761-9580. Medicare Part D Hospice Prior Authorization Information.
Certain medical services and treatments need approval before you receive care. Medicaid only BCCHP and MMAI. The form contains important information regarding the patients medical history and requested medication which Anthem will use to determine whether or not the prescription is included in the patients health care plan.
The members prescriber must obtain authorization from the Plan prior to dispensing the medication by a retail pharmacy or through mail order if applicable otherwise the medication. Fax - 1-855-476-4158 All requests for Vyvanse to Treat Binge Eating Disorder require a Prior Authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Lead Risk Assessment In addition to the state mandated required testing at ages one and two assessment of risk for high-dose lead exposure should be done at least annually for each child six months to six years of age.
An Issuer may also provide an electronic version of this form on its website that you can complete and submit electronically through the issuers portal to request prior authorization of a health care service. Medicaid Claims Inquiry or Dispute Request Form. UnitedHealthcare requires that care providers complete the notificationprior authorization process for genetic and molecular testing performed in an outpatient setting for UnitedHealthcare Community Plan members in these states.
Certain medications will require prior authorization to ensure the medical necessity and appropriateness of the prescription order as defined by Highmark prior authorization policies. Dupixent Prior Authorization Form. This will ensure that the care our members receive while living and traveling outside of the Highmark service area is medically necessary and managed.
Modafinil and Armodafinil PA Form. Maryland Michigan Missouri New York Tennessee and Texas. Highmark requires authorization of certain services procedures andor DMEPOS prior to performing the procedure or service.
 Free Prior Rx Authorization Forms Pdf Eforms
Free Prior Rx Authorization Forms Pdf Eforms
 Highmark Bcbs Medication Prior Authorization Form Fresh Free Form 2018 Uhc Prior Authorization Form Models Form Ideas
Highmark Bcbs Medication Prior Authorization Form Fresh Free Form 2018 Uhc Prior Authorization Form Models Form Ideas
Https Www Highmarkhealthoptions Com Content Dam Digital Marketing En Highmark Highmarkhealthoptions Providers Provider Resources Provider Forms Oct19providerforum Pdf
 Top 28 Blue Cross Blue Shield Prior Authorization Form Templates Free To Download In Pdf Format
Top 28 Blue Cross Blue Shield Prior Authorization Form Templates Free To Download In Pdf Format
Https Www Ibx Com Documents 35221 56677 Prior Auth Botulinum Toxins Pdf 99b5b638 Fc7c 290b Ab03 58c7a997ef40 T 1580924446000
Https Www Highmarkbcbswv Com Pdffiles Specialty Drug Request Fax Form Pdf
 Fillable Online Highmark Prior Authorization Forms Fax Email Print Pdffiller
Fillable Online Highmark Prior Authorization Forms Fax Email Print Pdffiller
 Drug Request Form Fill Online Printable Fillable Blank Pdffiller
Drug Request Form Fill Online Printable Fillable Blank Pdffiller
 Free Highmark Prior Rx Authorization Form Pdf Eforms
Free Highmark Prior Rx Authorization Form Pdf Eforms
Https Content Highmarkprc Com Files Region Pa Caremgmtprog Radmgmtprog Hm Prior Auth Guide Pdf
 Highmark Bcbs Medication Prior Authorization Form Best Of Anthem Express Scripts Prior Authorization Form New Free Gov Forms Models Form Ideas
Highmark Bcbs Medication Prior Authorization Form Best Of Anthem Express Scripts Prior Authorization Form New Free Gov Forms Models Form Ideas
 Highmark Bcbs Medication Prior Authorization Form Inspirational Free Resume Format Blue Cross Blue Shield Medication Prior Models Form Ideas
Highmark Bcbs Medication Prior Authorization Form Inspirational Free Resume Format Blue Cross Blue Shield Medication Prior Models Form Ideas
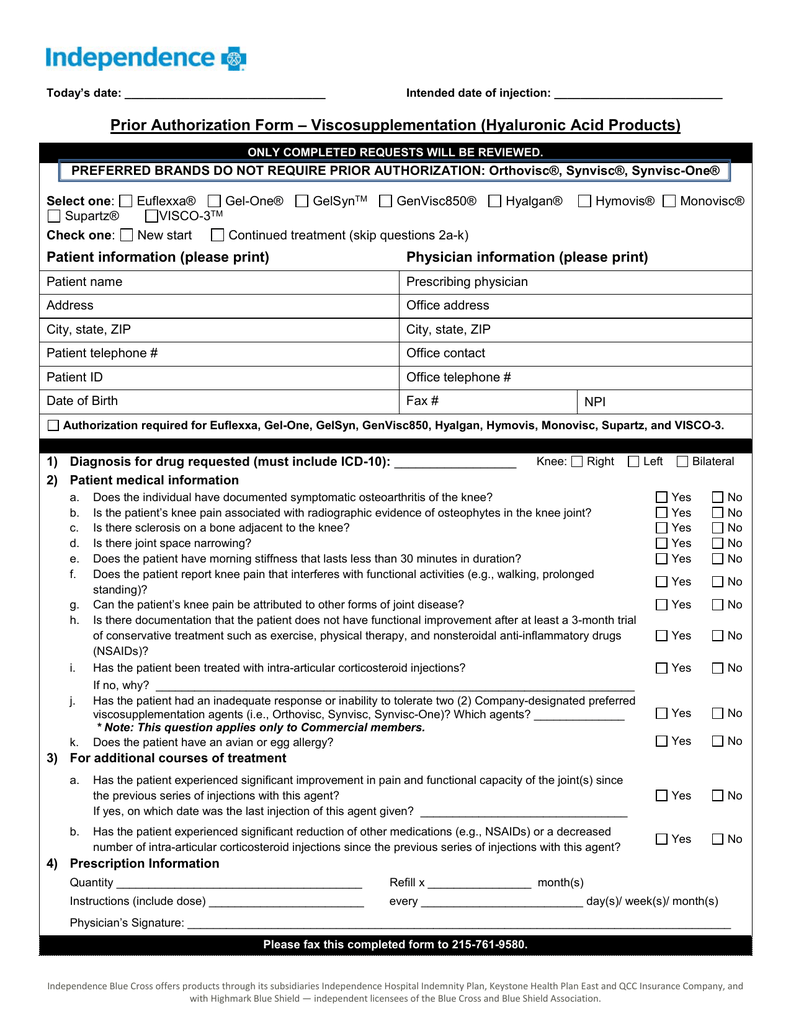 Prior Authorization Form Viscosupplementation Hyaluronic Acid
Prior Authorization Form Viscosupplementation Hyaluronic Acid
Highmark Bcbs Medication Prior Authorization Form Unique Free Form 2018 Aarp Prior Authorization Form Models Form Ideas




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.