Performance was calculated overall and stratified by COVID-19 test result sex age group 64. Z029 is a billablespecific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
 Using Icd 10 Cm
Using Icd 10 Cm
We used to use 0000 Misc for situations like this.

Icd 10 code for medical records review. The 2021 edition of ICD-10-CM Z029 became effective on October 1 2020. HEDIS consists of 75 measures. ICD-10-PCS has been designed systematically.
This is the American ICD-10-CM version of Z029 - other international versions of ICD-10 Z029 may differ. CHAPTER 3 Medical Records. The ICD-9 code set was replaced by the more detailed ICD-10 code set on October 1 2015.
Main Outcomes and Measures The sensitivity specificity positive predictive value PPV and negative predictive value NPV of ICD-10 codes for fever R50 cough R05 and dyspnea R060 were compared with manual medical record review. Dial 1-800-670-2809 for a Free Trial of our HEDIS medical record review services. We supply free records and warn patients if they have mutiple personal requests we would charged - but.
Codes abstracts and analyzes inpatient andor outpatient medical records using International Classification of Diseases Tenth Revision ICD-10. And use 99080 cpt code for medical records request- diagnosis code V700which doesnt make sense we force in the fee and payment thru the account records. Identify various medical reports important to the coding process.
2 ICD-10 Procedure Coding System ICD-10-PCS is a set of codes for medical proce-dures developed by 3M Health Information Sys-temsundercontracttotheCenterforMedicareand Medicaid Services of the US. Our skilled medical coding team assigns the correct NCQA-approved CPT and ICD-10 codes to indicate that well-care was provided so that HEDIS quality of care goals can be indicated through claims data. A joint effort between the healthcare provider and the coder is essential to achieve complete and accurate documentation code.
A baseline CDI record review is a concurrent review of an inpatient medical record in which the CDI specialist attempts to abstract key information for the purposes of quality measurement compliant coding and appropriate. In 2015 ICD-10-CM contains more than 141000 codes to report healthcare diagnoses and procedures. CPT CODE 99080 99090 99091 - special review codes Medical Billing and Coding - Procedure code ICD CODE.
You just make up a dummy code if you must have a dx code to bill out for the record review. These codes change over time so they have a number appended to them to show which set of codes is being used. Demonstrate the use of a CoderAbstract Summary Form and a PhysicianCoder QueryClarification Form.
The ICD codes are comprised of four or five characters with a decimal point. Medical Billing and Coding - Procedure code ICD CODE. The V codes are for indicating a patient or someone related to the patient encountered services with a physician.
Z7689 is a billablespecific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes. Demonstrate coding from medical reports by using the 10-step method. Persons encountering health services in oth circumstances The 2021 edition of ICD-10-CM Z7689 became effective on October 1 2020.
ICD codes are the codes that designate your diagnosis. Furthermore CAC includes a variety of computer-based approaches that do not require human interaction to transform narrative text in clinical records into structured text which may include assignment of codes from standard terminologies such as ICD-9-CM ICD-10-CMPCS CPTHCPCS and SNOMED CT. Each code consists of seven characters and the charac-.
Set UHDDS guidelines ICD-10-CM Official Guidelines for Coding and Reporting and internal documentation and coding policies. International Classification of Diseases Tenth Revision Clinical Modification ICD-10-CM Published by the World Health Organization WHO in 1999 and implemented in the US. ICD-10-CM is three to seven characters long and is entirely alphanumeric.
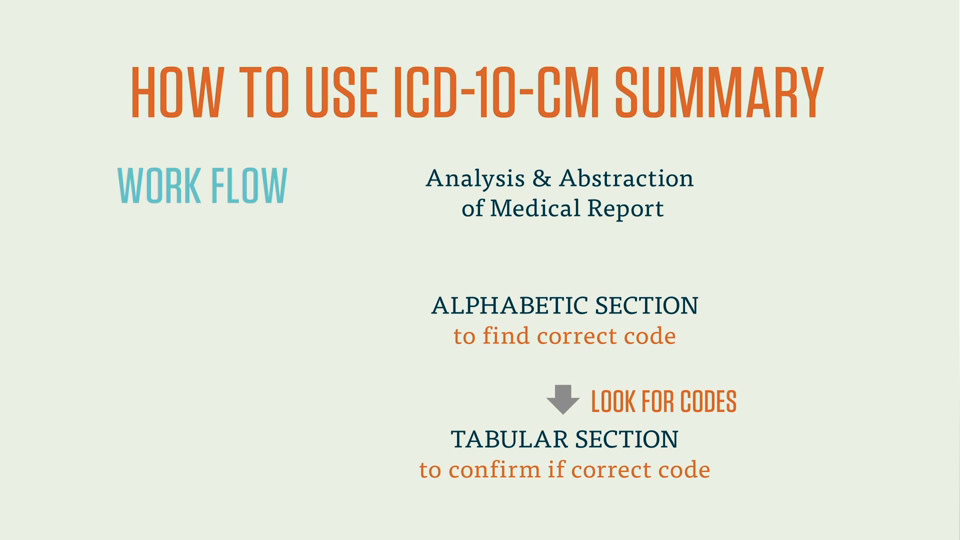
The Basis for All Coding 41 The coding process begins with a careful and strategic review of the medical record. The diagnosis codes Tabular List and Alphabetic Index have been adopted under HIPAA for all healthcare settings. Always coding to the highest level of specificity Identifies coding error eg incorrect primary diagnosis MCCs CCs and procedure codes and re.
CPT CODE 99080 99090 99091 - special review codes. However the article also warns. Under the Part B physician fee schedule through either automated medical review or complex medical record review based solely on the specificity of the ICD-10 diagnostic code as long as a physicianpractitioner used a valid code from the right.
S9981 Medical records copying fee administrative HCPCS Procedure Supply Codes S9981 - Medical records copying fee administrative The above description is abbreviated. Adherence to these guidelines when assigning ICD-10-CM diagnosis codes is required under the Health Insurance Portability and Accountability Act HIPAA. Hi - the only records weve ever billed are for third party requests- insurance work comp etc.



